Over the past hundred years, medicine has treated aging and cancer as two completely separate fronts. Aging researchers asked: why do our cells lose function over time? Cancer researchers asked: why do certain cells start dividing uncontrollably? The assumption was that these two questions are fundamentally different, and therefore require different therapeutic approaches.
But the wave of 2026 research reveals a different picture: zombie cells and cancer are two sides of the same biological coin. Cellular senescence, the process where a cell stops dividing but doesn't die, is both the body's first defense against cancer and the factor that accelerates tumor appearance in old age. This understanding, together with a fresh discovery about a vulnerability of senescent cells, opens a new therapeutic approach that exploits senescence as a double-edged weapon.
What are Zombie Cells and Cancer: A Dual Definition
To understand the new approach, one must recall what zombie cells are and their connection to cancer:
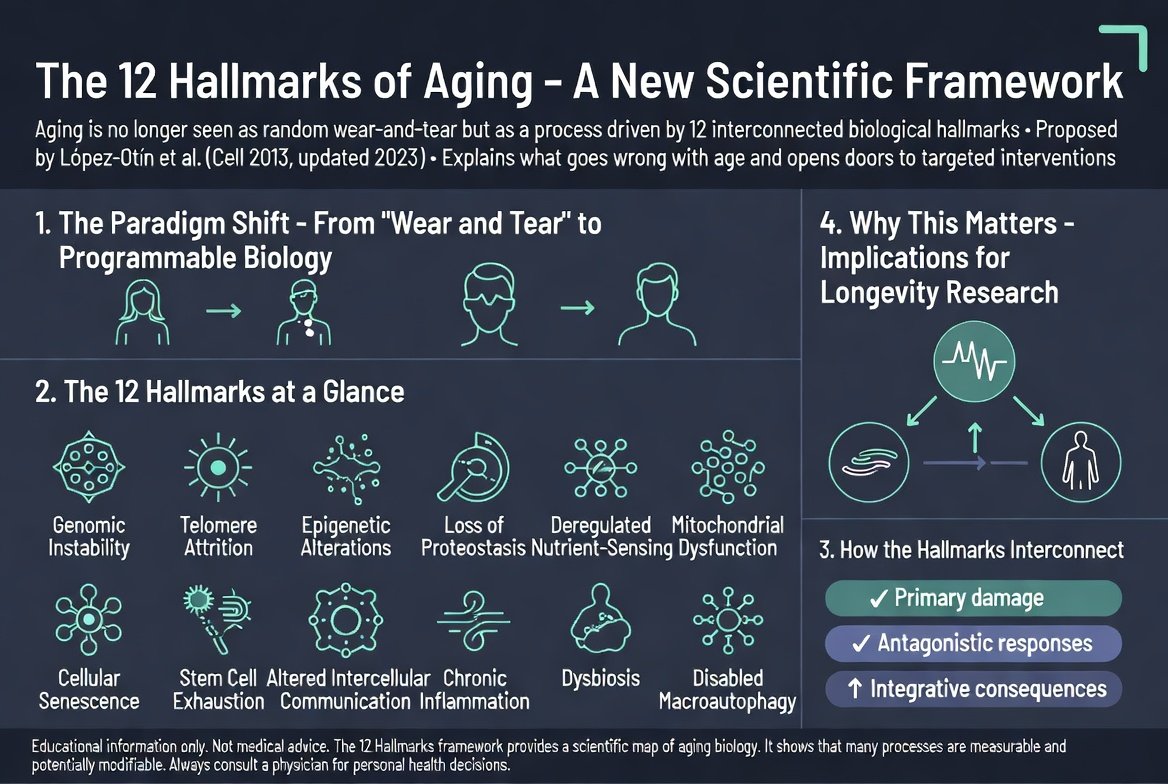
- Zombie cells (senescent): Cells that have stopped dividing due to DNA damage, oxidative stress, or telomere attrition. They don't die, don't divide, and secrete inflammatory substances called SASP.
- Senescence as an anti-cancer mechanism: When a cell acquires a dangerous mutation, its natural genes (like p53 and p16) may trigger senescence. This prevents the cell from becoming a tumor.
- The paradox: Over time, senescent cells accumulate. Their inflammatory secretion damages neighboring tissues and the immune system, creating an environment that actually promotes tumor growth.
- Cancer itself can undergo senescence: Chemotherapy and radiotherapy cause some cancer cells to enter senescence instead of dying. Such cells can later awaken and cause recurrence.
This connection is far more complex than 'zombie cells cause cancer.' Senescence is both a protector and a threat, depending on timing and context.
2026 Discovery: The Achilles' Heel of Zombie Cells
In a study published in the journal Nature Cell Biology in April 2026 (D'Ambrosio and colleagues), researchers screened a library of over 10,000 electrophilic molecules and looked for compounds that selectively kill senescent cells. They discovered that senescent cells are in a state of high oxidative stress and high iron levels, making them particularly vulnerable to a destruction process called ferroptosis, a cell death driven by lipid oxidation.
To survive, senescent cells rely on a single protective enzyme called GPX4, which neutralizes oxidized lipids. The researchers showed that when GPX4 is blocked (or using the senolytic compounds identified in the screen), senescent cells are selectively killed by ferroptosis, while healthy cells are less affected. In combination with anti-cancer treatments, blocking GPX4 eliminated senescent tumor cells in models of melanoma, prostate cancer, and ovarian cancer. This is a specific vulnerability that turns cellular aging itself into a therapeutic target.
The Connection to Senolytic Oncology: Two Opposing Approaches
Two strategies are developing in parallel in the field, targeting different sides of the same biology.
First Approach: Clearing Senescent Cells to Prevent Cancer
This approach is based on the insight that senescent cells in old age create a chronic inflammatory environment that encourages mutations and promotes tumor development. The solution: administer senolytic drugs that identify and eliminate senescent cells, thereby clearing the 'pre-cancerous field' before a tumor even appears.
Drugs like dasatinib + quercetin (D+Q) and fisetin have shown in preclinical mouse studies the ability to reduce the senescent cell burden and improve health metrics. It is important to emphasize: the ability of such clearance to reduce cancer incidence in humans has not yet been proven in randomized controlled trials. This is a promising rationale based mainly on animal models.
Second Approach: Inducing Senescence in Cancer Cells and Then Clearing Them
This is the opposite approach. Instead of preventing cancer, it treats existing cancer. The idea: administer a drug that forces senescence on active cancer cells, turning them from 'uncontrollably dividing tumor cells' into 'non-dividing zombie cells.' Then, administer a senolytic drug that clears the newly formed senescent cells.
This approach is called the One-Two Punch. The first step (induction) freezes the tumor in place. The second step (clearance) eliminates it. The advantage: cancer cells resistant to standard chemotherapy are often still sensitive to senescence induction. The concept was extensively reviewed in a major review in the journal Nature Reviews Cancer (Wang, Lankhorst, and Bernards, 2022).
Current Evidence
Pancreatic Cancer: Inducing Senescence and Altering the Environment
In a landmark study published in Cell in 2020 (Ruscetti, Morris, Lowe, and colleagues), researchers tested the approach in a mouse model of KRAS-mutant pancreatic cancer, one of the deadliest cancer types. They combined trametinib (a MEK inhibitor) with palbociclib (a CDK4/6 inhibitor) to induce senescence in cancer cells. The combination caused remodeling of tumor blood vessels and improved immune cell infiltration and immune response. However, the effect as a standalone treatment for pancreatic cancer was limited, and the main value was in creating vulnerabilities that could be exploited in combination with immunotherapy. This is a demonstration of the principle, not a ready-made drug.
Fisetin as a Senotherapeutic: Health and Lifespan
Mayo Clinic researchers, led by James Kirkland, published in 2018 in the journal EBioMedicine (Yousefzadeh and colleagues) that treating aged mice with fisetin reduced senescence markers in several tissues, improved tissue health, and extended median and maximum lifespan. This establishes fisetin as a genuine senotherapeutic, but the study focused on health and lifespan, not cancer incidence. There is no experiment here showing a numerical decrease in tumor rate, and it is important not to present it otherwise.
One-Two Punch: Senescence Induction Followed by Senolytic
A study published in Molecular Oncology in 2020 (Saleh and colleagues) demonstrated the 'two-hit' principle: cancer cells driven into senescence by chemotherapy (etoposide or doxorubicin) were subsequently eliminated using the senolytic navitoclax (ABT-263), which interferes with the interaction between BCL-XL and BAX proteins, pushing cells into apoptosis. In animal models, administering navitoclax after chemotherapy led to more prolonged tumor suppression. This is a preclinical proof-of-concept for the senescence-induction followed by clearance sequence.
The Comprehensive Review
The major review in Nature Reviews Cancer (Wang, Lankhorst, and Bernards, 2022) summarizes the one-two punch approach and the preclinical evidence supporting it. Among the examples it brings: combining a PARP inhibitor (olaparib) with the senolytic navitoclax in an ovarian cancer model, and combining a CDC7 inhibitor (XL413) to induce senescence in p53-mutant cells followed by an mTOR inhibitor to eliminate senescent liver cancer cells. The review clarifies that this is a promising but still largely preclinical approach, not a uniform number of 'response doubling.'
What About Specific Cancer Types?
The dual-action approach is not equally suitable for all cancer types. Here is where it looks most promising and less so, based on preclinical research:
- Melanoma, Prostate Cancer, Ovarian Cancer: Here it was directly demonstrated that blocking GPX4 in combination with anti-cancer treatment eliminated senescent tumor cells (2026 study).
- Pancreatic Cancer: The approach caused blood vessel remodeling and improved immune response, but its effect as a standalone treatment was limited. An active research area.
- Hormone-Resistant Breast Cancer: CDK4/6 inhibitors are already used clinically. Adding a senolytic after them seems a natural direction to test.
- Leukemias: The senolytic drug dasatinib was originally developed for leukemia. Theoretical synergy exists.
- Lung Cancer: Promising, but complex due to tumor heterogeneity.
- Brain Cancer (Glioblastoma): Limited success, due to the blood-brain barrier hindering drug delivery.
- Castration-Resistant Prostate Cancer: Mixed results. In some cases, senescence actually contributed to resistance.
Should We Start Taking Senolytics?
This is the critical question, and it has several layers to understand.
If You Are a Healthy Person with No Cancer History
The evidence for cancer prevention with senolytics is based mainly on mice. In humans, there are no large randomized controlled trials yet proving that clearing zombie cells reduces cancer risk. Human studies of fisetin and D+Q are currently being conducted mainly for other conditions, and results regarding cancer are still far off. Caution is advised.
If You Are a Cancer Patient Undergoing Active Treatment
Do not take senolytics on your own. Timing is critical in the dual approach. A senolytic before the senescence induction phase can harm the treatment. Only an oncologist can correctly time the combination. It is important to remember that there is no published clinical trial in humans of the one-two punch approach in oncology, so this is a research field, not standard treatment.
If You Are a Cancer Survivor
This is a complex population. Senescent cells can remain after chemotherapy and cause late recurrence. Senolytics theoretically offer an option to eliminate them, but safety in survivors has not yet been proven in large trials. Talk to your oncologist before starting any supplement.
Side Effects and Risks
First-generation senolytics (dasatinib) are prescription drugs with non-trivial side effects, including nausea, fatigue, electrolyte disturbances, and temporary immune function decline. Fisetin is a supplement considered relatively safe, but the high doses used in studies (on the order of 1500-2000 mg per day in short cycles) differ from doses in commercial supplements, and they are also tested under supervision.
Additional Drugs in Development: What's Really Happening
It is important to distinguish between promise and result. Two 'next-generation' senolytic drugs that made headlines illustrate this:
- UBX0101: A senolytic developed by Unity Biotechnology. It failed in a Phase 2 trial for knee osteoarthritis (did not meet the primary endpoint), and its development for this indication was halted. It was never a drug for cancer prevention.
- FOXO4-DRI: An experimental peptide that releases the p53 protein from the FOXO4 protein and pushes senescent cells into apoptosis. It showed interesting results in mice, but it remains an experimental research tool, not an approved drug.
The lesson: even elegant ideas sometimes fail in the clinic, and the path from the lab to the patient's bedside is long and uncertain.
What to Take Away from the Research?
- Understand that senescence is not just 'bad'. It is the body's first defense against cancer. The goal is not to eliminate all senescence, but to manage it wisely according to stage and timing.
- If diagnosed with cancer, ask about clinical trials in the field of senescence and senolytics. Leading research centers are testing such approaches. Ask your medical team for a referral to a center involved in advanced clinical trials.
- Support your body's natural senescence. Intermittent fasting, physical activity, and adequate sleep all support mechanisms that identify problematic cells and either push them into senescence or eliminate them.
- Adhere to routine screening tests. Early detection of tumors remains the most important tool for preventing mortality. Mammography, colonoscopy, PSA, skin checks, and for smokers, lung scans.
- Don't believe advertisements for 'miracle senolytic' supplements. Most of what is sold commercially is not yet proven. Fisetin is an exception with early studies, but it also requires a high and monitored dose.
- If you are in a family with a genetic predisposition to cancer (BRCA1/2, Lynch syndrome, etc.), talk to a specialist doctor about the possibility of joining prevention studies.
The Broader Perspective
The dual-action approach to zombie cells and cancer signifies a conceptual shift. For a hundred years, cancer medicine was in direct warfare: identify the cancer cell, eliminate it. Now, we are learning to change the battlefield: reshape the cellular environment so that tumors find it difficult to appear and survive.
The central understanding is simple: cancer is largely a disease of aging, and treating it requires an understanding of aging biology. About 60% of new cancer cases are diagnosed in people over 65, and age is the strongest risk factor for most cancers. Medicine that ignores this connection misses vital opportunities.
The vision of exploiting senescence as a weapon against cancer is to gradually turn cancer from a deadly disease into a more manageable one. Not just to eliminate tumors when they appear, but to slow their onset, and prevent recurrence after treatment. However, it is important to end honestly: most of these approaches are still preclinical or in very early stages, and there is no approved oncological treatment based on the senescence-induction and clearance sequence. This is a promising direction, not a promise.
The big lesson: biology is not separate fields. Zombie cells, which a decade ago were considered marginal in the field of aging, are now at the heart of cancer research. When basic research merges with advanced medicine, breakthroughs emerge that would not have been possible in each field alone.
References:
Nature Cell Biology - Electrophilic compound screening identifies GPX4-dependent ferroptosis as a senescence vulnerability (D'Ambrosio et al., 2026)
Nature Reviews Cancer - Exploiting senescence for the treatment of cancer (Wang, Lankhorst & Bernards, 2022)
Cell - Senescence-Induced Vascular Remodeling Creates Therapeutic Vulnerabilities in Pancreas Cancer (Ruscetti et al., 2020)


💬 Comments (0)
Be the first to comment on the article.